Implant type
There are both saline filled and silicone gel filled implants available. There is no evidence that silicon is harmful or can cause disease outside the breast, and most modern implants have an outer silicone shell even if they are filled with saline. Many implants are now made of “cohesive” silicone gel. While this feels soft, it has a structure like a jelly cube, so cannot leak out into the breast tissues as easily as the older liquid silicone implants.


Implant Size
The correct implant size depends on a combination of factors – your desired size after surgery, the size of your chest, whether your breast sit high up or lower down on your chest and your degree of ptosis. It is usually helpful if you can bring some pictures of women who have the sort of proportions and shape you wish to achieve, so we can agree on your aims. There is also a very useful technique you can use at home to try and work out how much larger you want to be.
Silicone shell sizers
During your consultation you will have the opportunity to see an approximation of your final result with the use of silicone shell sizers. You may find it useful to bring a non padded bra in your desired cup size to these consultations for this purpose.
Positioning of the implant
The implant can be placed directly under the breast in a subglandular position or under the muscle of chest wall, the subpectoral position. A technique known as the “dual-plane” can be used which combines the two, and may help correct ptosis while at the same time increasing tissue coverage over the upper part of the implant. Every woman obviously represents an individual case and we will discuss the various advantages and disadvantages of each approach for you personally.
Who chooses to have breast reduction?
Most women who desire a breast reduction simply feel that their breasts are disproportionately large and heavy. For many women this makes it difficult to find clothes which fit properly, particularly dresses. Some women with large breasts develop “shoulder grooving” from the bra straps, and rashes under the breasts in hot weather. Others complain of back and neck pain and feel that the heaviness of their breasts is causing postural problems.
Some women develop very large breasts during puberty; others find that their breast size increases after having children or following the menopause.
A breast reduction will not prevent breast pain, as there is still plenty of breast tissue left after the operation, but some patients find that the heaviness associated with their pain is better after surgery.
A breast reduction will not prevent you getting breast cancer, though there is some evidence that reducing the amount of breast tissue can reduce the risk of cancer slightly. It is important to remember that mammograms will be less accurate after a reduction because the scar tissue inside the breast can mask a very small cancer, and you should tell your mammographers that you have had reduction surgery.
For more information from the Association of Breast Surgery, BAPRAS and BAAPS websites on breast reduction.
Preoperative Assessment
During the initial consultation I will discuss with you your reasons for wanting a reduction, and how much smaller you would ideally like to be. It is not possible to guarantee a particular bra size afterwards, due to the different ways bra size is calculated. The procedure is designed to make your breasts proportionate with your trunk, so the final size will depend to some extent on your overall size.
I will discuss with you the risks and complications of breast reduction surgery and what to expect afterwards. You will be shown photographs of the procedure and the results. There are several different methods of performing a breast reduction and I will discuss which of these are appropriate for you.
If you are 40years or older a preoperative mammogram will be ordered.
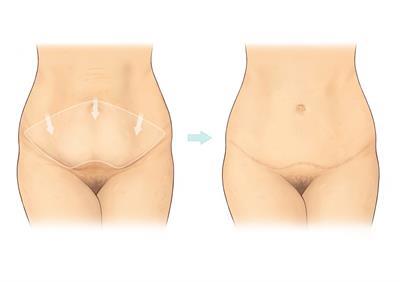
Types of Breast Reduction
Although it is possible to reduce breast size in some women by liposuction alone, I do not generally advise this, as it dos not incorporate any form of uplift, and so does not give very good overall results.
In small-breasted women who need a small reduction in order to improve symmetry, then it is sometimes possible to use the Benelli technique, which leaves only a scar around the areola, the pigmented skin around the nipple. This type of reduction does not work for moderate or large breasts.
The commonest type of breast reduction performed in the UK is the inverted T, or Wise pattern, technique, which leaves a scar around the areola, down to the crease under the breast and along the crease from end to end. Like the Benelli, this technique is dependent on the breast skin to hold the shape of the breast. Over time, the skin tends to stretch and the breast “bottoms out”, leaving most of the breast tissue sitting below the level of the nipple, rather than behind it. In extreme cases, this can lead to difficulty wearing a bra, as the high-riding nipple is pushed out of the top of the bra cup.

What You Really Need to Know About Breast Lifts
Click here for BAAPS guide for patients
Can I have a breast lift and not have implants?
A breast lift without implants works well in patients who are satisfied with their breast size but not satisfied with sagging and excessive overhang of their breasts and a low nipple position. A breast lift will reshape the breast, raising the nipple to a better position and reducing the overhang of the breast. The breast will not be smaller than it was before, just higher. There will be better fullness of the breast behind the nipple as the tissue is pushed upward and held in a tighter “skin envelope”. However, there is no way of reliably creating more fullness in the upper pole of the breast without using an implant. And since the scars of a breast lift are in the lower breast and hidden beneath a bathing suit, a lift will not tighten the loose skin of the upper breast; only restoring volume with an implant will fill out a truly deflated breast.
I just want implants. Why would I need a breast lift too?
Many patients who want to increase their breast size and fullness with implants want to avoid the additional scars of a breast lift. However, if the breast is too low and too overhanging past the crease under the breast, this skin and tissue will not be properly filled out by the implant and may have the appearance of “hanging off” the implant. This is also called a “double bubble” or “Snoopy” breast. This is because the bottom of the implant pocket is at this infra-mammary crease. If the breast hangs too low past this point, the implant will have little effect on filling it out. And if the nipple is low, it may become even more down pointing as it is too far below the midpoint or “equator” of the implant.
In summary, breasts implants do not lift breasts, they fill them out where they are. And if the breast hangs too low, they won’t even do that very well.
How can you tell if I need a breast lift in addition to implants?
When the surgeon examines you, measurements are made to assess where the nipple lies in relation to the fold under the breast, and how much breast overhang if any there is past this fold.
There are some patients whose breasts are “borderline” in terms of whether a breast lift is needed. The nipple may be somewhat lower than ideal, and there may be more breast overhang than ideal but not too excessive. In many cases a “dual plane” technique may be used in order to obtain a good result without the additional scars of a lift. This involves placing the implant under the muscle, as is usually done for better implant camouflage and a lower risk of capsular contracture, but releasing the attachment of the muscle to the overlying breast tissue a little to encourage the implant to “fill out” the loose tissue at the bottom of the breast. If this is successful, the nipple may look a little higher (even though it is not) as the bottom of the breast is filled by the implant. In this way, some of these borderline patients may avoid a breast lift. But if they want a higher breast or higher nipples, they will need a lift.
Why are there different types of lift and different scars with each one?
The breast lift with the least scarring is the periareolar or Benelli breast lift, which has a scar just around the areola and no vertical scar. In this lift a larger circle is drawn out from the areola, the top of this outer circle placed where the areola will be raised, and an inner circle is drawn within the areola (designed to reduce the size of a stretched-out areola). The skin between is removed, a purse-string suture is placed at the outer circle and cinched down around the inner, smaller circle, thus tightening the skin, reducing the areola size, and raising the nipple position.
Although most patients who need a lift want to avoid the vertical scar, there are serious limitations to this periareolar lift. If anything more than a very mild lift is required, the cinching down of this larger circle creates a gathering, puckered effect that leads to unsatisfactory scarring. Also, this tightening can lead to flattening of the breast shape that even an implant will not help counteract. (This lift is usually not attempted in patients without an implant, as the flattening effect and very minor lifting effect is not enough to obtain a good result.) Also, there is less control over the final size and shape of the areola, since late stretching of the areola can occur even with a permanent purse-string suture.
The vertical breast lift adds a vertical scar to this periareolar lift. This vertical scar has a very strong and effective shaping effect on the breast. A periareolar purse-string suture is still used, but closing the vertical incision reduces the size of the large outer circle and reduces the gathering effect. There is a difference of opinion among surgeons as to how effective this type of lift is at reducing significant breast overhang.
The anchor breast lift consists of a scar around the areola and a vertical scar, and adds a scar under the breast that allows very effective lifting and reduction of breast overhang. Moreover, the skin removal that raises the nipple to a better position and reduces the areola size does not require the dependence on a purse-string gathering suture; instead, skin is trimmed in a keyhole pattern than closes around the newly reduced areola with an exact fit. Thus the control over areolar size and shape is the most reliable, and the periareolar scar is of the best quality. Many surgeons believe this is the most effective breast lift with the best scar quality.

Can I have a breast lift and breast augmentation at the same time?
This is a controversial topic. Some surgeons never perform these at the same surgery, while others always do. Essentially, these two procedures can “work against” each other: breast augmentation expands the breast while a breast lift tightens the breast. You might think that you could place an implant and just “tailor” and trim the skin around it. Unfortunately, a certain amount of skin removal is required in order to lift the nipple to the correct position, close the defect where the nipple and areola used to be (and large areolas make this even tighter!), and adequately reduce the overhang of the breast. The tightness of this skin removal can restrict the size of an implant that can be safely placed, and this can be smaller than the patient desired. With too tight a closure, incisions can come apart, skin can lose its blood supply and die, healing can be prolonged, and the scars that result can be very wide and unsightly.
Another issue is the blood supply to the nipple. Dissecting a pocket for an implant can reduce the blood supply to the nipple, as can the dissection required to move the nipple higher as part of a breast lift. When performed separately, it would be extremely rare to have any blood supply issues; when performed together, this could tip the balance and loss or necrosis of the nipple and areola has been known to occur, especially with larger implants, tighter closures, and in patients with thinner tissues.
In general, patient who require minor lifts and have thicker tissues can often have both procedures performed at the same time, while patients with thinner tissues who need more major lifts may be safer having the lift performed first and the implant placed later. This staged approach takes a loose, overhanging breast that is not a good candidate for an implant, and reshapes the breast so that, once healed, it becomes a good candidate for breast augmentation.
No one wants extra scars that are not necessary, but many breast augmentation patients try to avoid a breast lift at all cost even when it is needed. This sets them up for a poor result and more surgical procedures in the future. Some surgeons will place too-large implants above the muscle in an attempt to fill out the loose skin and avoid the breast lift that the patient needs but does not want. Ultimately this may lead to even more tissue stretching and breast sagging, and require more complex surgeries to fix the problem. It is better to have a well-shaped breast with scars that generally fade nicely over time than an implanted breast with an unsatisfactory shape and contour.